A rare oral blood blister managed with chlorhexidine and benzydamine mouthwashes
A recently published case report highlights the supportive use of chlorhexidine and benzydamine mouthwashes in a patient with angina bullosa hemorrhagica, a rare oral blistering condition that may initially appear alarming to both patients and clinicians.
Angina bullosa hemorrhagica (ABH) is a benign disorder characterised by the sudden formation of blood-filled blisters on the oral or oropharyngeal mucosa. It mainly affects middle-aged and older adults and may be mistaken for a bleeding disorder, autoimmune vesiculobullous disease, infection, or malignancy.
ABH is commonly triggered by minor mechanical trauma, such as chewing hard food or undergoing a dental procedure. Diabetes, hypertension, and previous or ongoing use of inhaled corticosteroids may also increase mucosal fragility.
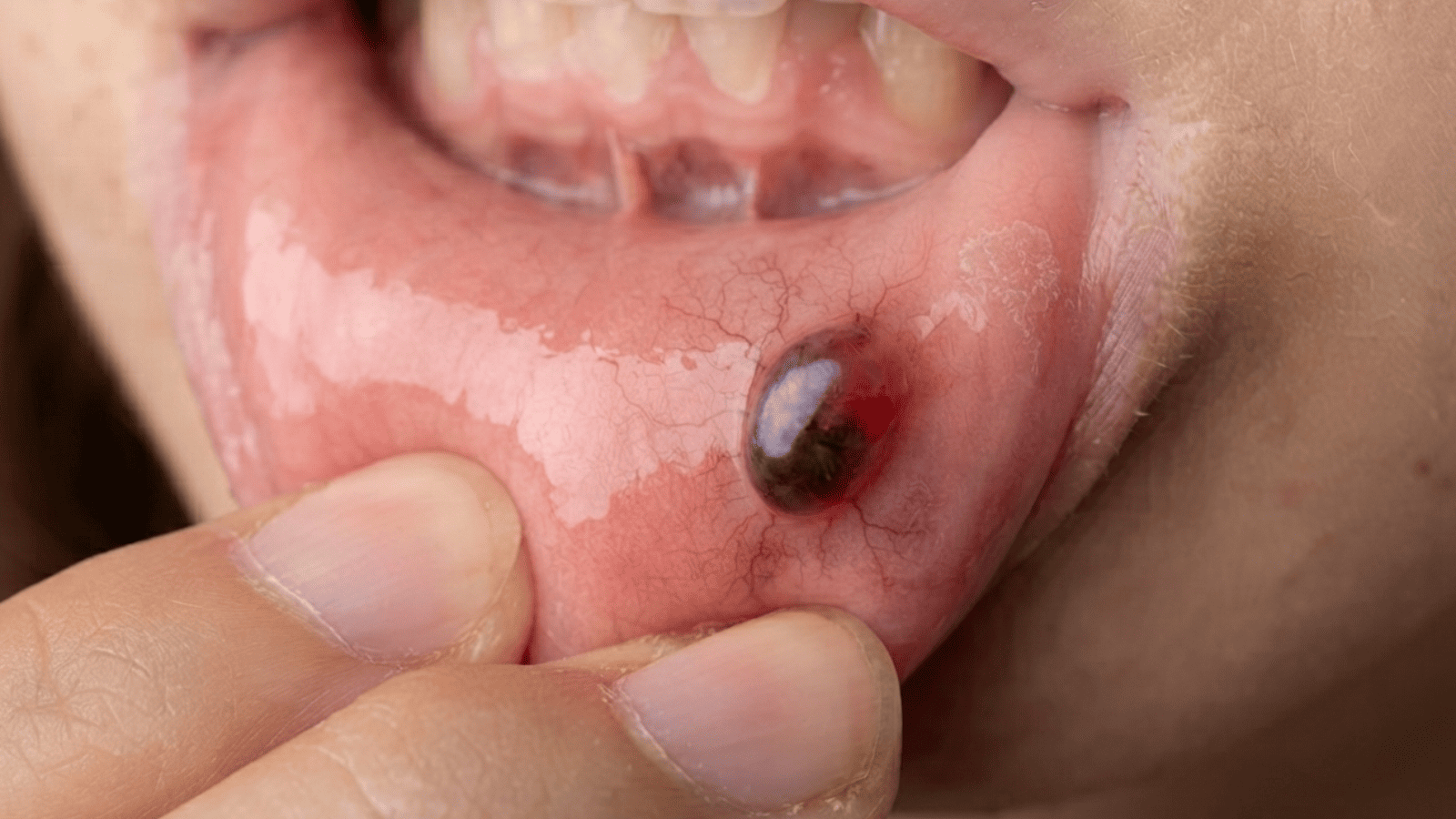
The reported case involved a 55-year-old woman who developed a painful, dark red-to-purple blister on the ventral surface of the tongue after eating. The blister ruptured spontaneously within a few hours, leaving a shallow erosion with burning discomfort. She had experienced two similar episodes during the previous six months, both associated with trauma from hard foods.
Diagnosis is primarily clinical. Important clues include sudden onset, an exclusively oral lesion, a preceding traumatic event, rapid rupture, recurrence, normal platelet and coagulation findings, and complete healing without scarring. In this case, complete blood count, prothrombin time, and partial thromboplastin time were normal. The absence of skin lesions, fever, lymphadenopathy, and other systemic signs helped exclude autoimmune, infectious, and haematological disorders.
Management of ABH is generally conservative because the lesion usually heals spontaneously. Benzydamine hydrochloride mouthwash was used to reduce pain and burning, while 0.12% chlorhexidine mouthwash provided local antimicrobial support and helped minimise the risk of secondary contamination after rupture. Pain subsided within three days, and complete epithelialisation occurred by day seven without scarring.
ABH usually resolves within 7–14 days. Early recognition, reassurance, and appropriate supportive care can prevent unnecessary biopsy or surgical intervention. Persistent, extensive, recurrent, or atypical lesions should be investigated further.
Reference:
Khajehzadeh F. Angina Bullosa Hemorrhagica: A Rare Case Involving the Ventral Tongue. Clin Case Rep. 2025 Dec 29;14(1):e71748. doi: 10.1002/ccr3.71748. PMID: 41476808; PMCID: PMC12747858.