

As dentists, we are often taught a rigid equation regarding periodontitis and occlusion: Inflammation + Occlusal Trauma = Accelerated Destruction.
The standard protocol suggests we must address both to stop tissue loss. But clinically, this is difficult. We often face patients with “high points” or deflective contacts who are in pain, anxious, or possess inflamed, bleeding gums that make accurate occlusal analysis impossible.
Do you pick up the bur and grind immediately? Or do you wait?
A breakthrough 2025 study published in Bioengineering suggests a paradigm shift: You can buy time.
By using Chlorhexidine (CHX) to control the “inflammation” variable, you can stabilize the periodontium for up to three months—even if the traumatic forces remain active.
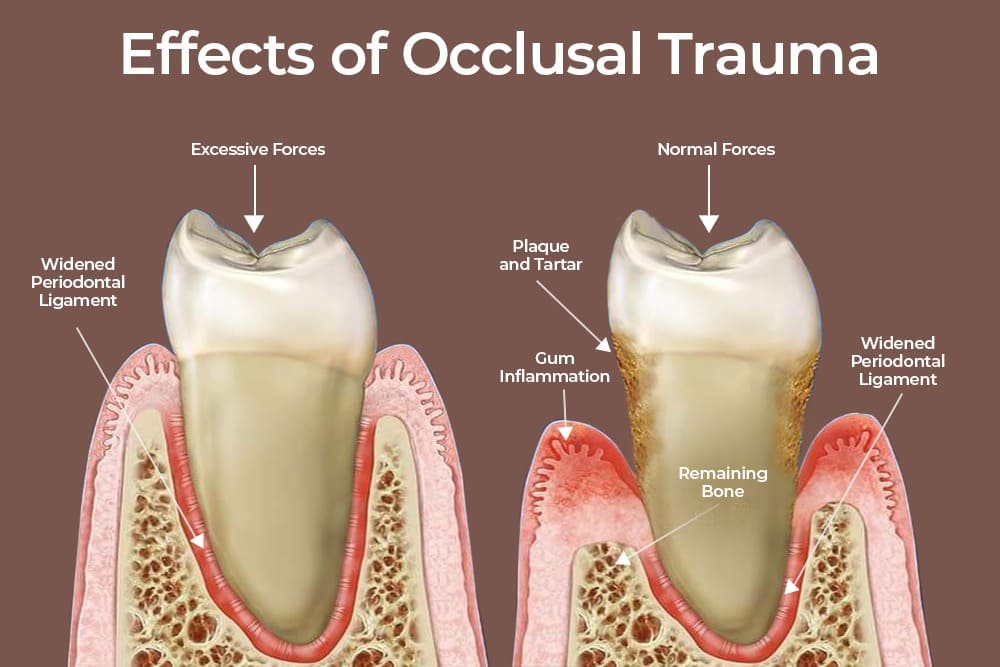
We know that while occlusal trauma does not initiate periodontitis, it accelerates attachment loss in teeth with compromised support. When a patient presents with combined periodontal inflammation and occlusal disharmony, immediate occlusal adjustment isn’t always feasible. The patient might be:
The study tracked 52 patients with confirmed deflective occlusal contacts. Crucially, no occlusal adjustments were made during the observation period. One group used CHX mouthwash, and the other did not.
The results were eye-opening for daily practice:
Based on this data, here is an evidence-based protocol for stabilizing these complex cases using the “Stabilization Bridge” approach:
This research gives us a new tool: Phased Therapy.
You do not always need to rush into irreversible occlusal adjustments on day one. Use a 0.12% or 0.2% CHX mouthwash to “put out the fire” of inflammation first. This reduces the microbial load and gives you a 3-month window of relative stability.
During this stabilized period, you can build patient trust, reduce anxiety, and plan for the necessary mechanical adjustments or restorative work with a clearer clinical picture.
Think of Chlorhexidine not just as an antiseptic, but as a strategic tool to buy stability in your most complex occlusal cases.
Nicolae XA, Preoteasa E, Murariu Măgureanu C, Moraru R, Preoteasa CT. Evolution of CPITN Index in Relation to Chlorhexidine Mouthwash Use in Patients with Deflective Occlusal Contacts. Bioengineering (Basel). 2025 Oct 22;12(11):1140. doi: 10.3390/bioengineering12111140. PMID: 41301097; PMCID: PMC12649252.

| PRODUCTS | QTY | PRICE | VALUE in INR |
|---|
| PRODUCTS | QTY | PRICE | VALUE in INR |
|---|